
The Pentagon Wants to Test Troops’ Testosterone. Here’s What the Science Actually Says.
The Pentagon's new testosterone screening policy has sparked debate. Here's what medical research actually says about testosterone, aging, and TRT.

Share
July 17, 2026
The Pentagon's new testosterone screening policy has sparked debate. Here's what medical research actually says about testosterone, aging, and TRT.
Share
This week, Defense Secretary Pete Hegseth announced a new Pentagon policy requiring service members ages 30 and older, regardless of gender, to be screened annually for “testosterone deficiency” as part of their existing periodic health assessment. Troops under 30 can request the test voluntarily. Screening will be mandatory; any resulting treatment, including testosterone replacement therapy (TRT), will be optional. Hegseth framed the initiative, branded as High-T, as a way to keep the force on “the leading edge of lethality.”
Beyond the military, TRT has grown substantially, with prescriptions rising to more than 11 million in 2024—compared with 7.3 million prescriptions in 2019, according to the monthly journal U.S. Pharmacist.
Testosterone is the primary sex hormone in men, produced mainly by the testes and regulated by a feedback loop between the brain and the testicles. It drives puberty and the development of secondary sex characteristics, and throughout adulthood it supports muscle mass and strength, bone density, red blood cell production, fat distribution, sperm production and libido. It also plays a role in mood and energy, though its influence there is smaller and harder to isolate than internet wellness culture tends to suggest. Testosterone isn’t exclusively a male hormone, either. Women produce it too, via the ovaries and adrenal glands, where it contributes to libido, energy, mood and bone maintenance.
Testosterone levels tend to fall by roughly 1 to 2 percent a year after age 30, but the decline is less uniform. One widely cited Endocrine Society study found that testosterone reductions over time were linked less to aging itself than to weight gain, smoking, depression and other modifiable health factors.
Married men, for example, showed smaller declines than unmarried men, likely reflecting broader differences in health behaviors rather than marital status itself. A separate lifespan-modeling study found that average total testosterone falls in a man’s 20s and 30s but showed no clear further decline through much of later adulthood—even as individual variation grows wider.
What the science doesn’t support is treating one number on a lab report as a measure of anyone’s fitness to serve, lead a classroom or do their job.
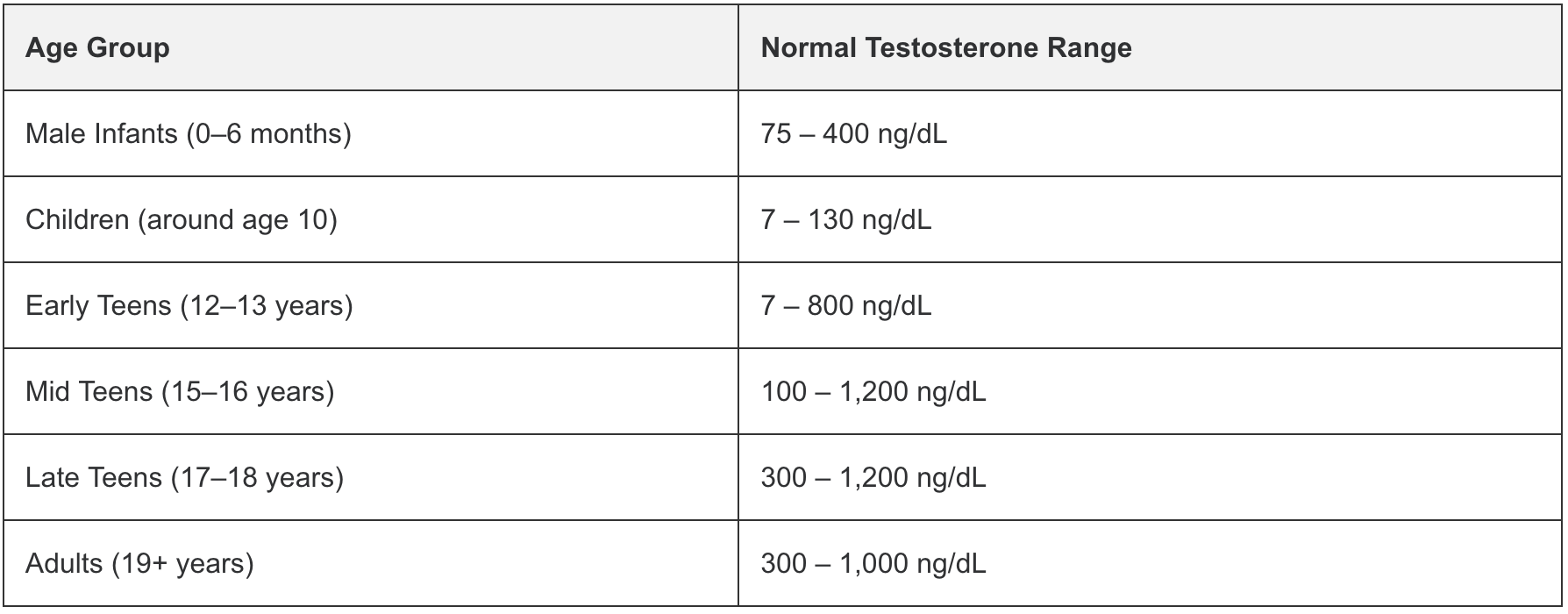
There’s also no single number that defines “normal.” Reference ranges vary by lab and typically span 300 to 1,000 nanograms per deciliter for adult men—a wide enough band that where you fall can shift with the time of day you’re tested, how much sleep you had and which lab ran the sample.
This is the piece that tends to get lost in High-T branding: A genuine testosterone deficiency, or hypogonadism, isn’t diagnosed from a single blood draw. Medical guidelines call for symptoms like persistent fatigue, low libido, erectile dysfunction, depression or unexplained muscle loss, paired with at least two separate early-morning readings confirming a low level. Estimates of how many men actually meet that bar vary, from around 2 percent to just over 5 percent, depending on the population studied and where the cutoff is drawn.
That distinction matters because testosterone prescribing has climbed sharply in recent years, and the American Urological Association has raised concerns that up to a third of men on TRT never met the clinical criteria for a diagnosis in the first place. Unnecessary TRT isn’t a neutral intervention; it can suppress the body’s own hormone production and fertility, thicken the blood and carry cardiovascular risks that researchers are still working to fully understand.
Reporting on the Pentagon’s new policy has also noted that its High-T framing borrows language more familiar from fitness influencers than from clinical medicine—a reflection of a broader cultural moment, encouraged by recent federal moves to loosen TRT prescribing restrictions.
For teachers and school staff, it’s a reminder that low or high testosterone content is a growing part of the online ecosystem many adolescent boys are exposed to, often stripped of nuance.
For physicians and nurses, this news cycle likely means more patients—military-affiliated or not—walking in asking about their testosterone levels. For teachers and school staff, it’s a reminder that low or high testosterone content is a growing part of the online ecosystem many adolescent boys are exposed to, often stripped of nuance.
It’s also a chance to separate a genuinely useful piece of preventive medicine—screening that can catch real hormonal problems tied to diabetes, obesity or pituitary issues—from a framing that treats a hormone level as a referendum on someone’s readiness, strength or worth.
Testosterone is a real hormone that does real things in the body, and screening for deficiency, done thoughtfully and paired with symptoms, is legitimate medicine. What the science doesn’t support is treating one number on a lab report as a measure of anyone’s fitness to serve, lead a classroom or do their job.
Join Dr. Vin Gupta—pulmonologist, public health expert, and professor—for a yearlong series offering expert-led webinars, blogs, resources, and Q&A sessions on pressing health issues to help AFT members and communities stay informed and healthy. Access all on-demand town halls and register for the next one.
Share My Lesson has curated a collection of resources and free lesson plans that will help educators and parents teach students about living healthy and active lives.







